
Punstoppable
A list of puns related to "Tryptophan hydroxylase"
Tryptophan 6g+Tryptophan hydroxylase inhibitors(Inhibitors of creation serotonin from Tryptophan)+MAOI=DMT microdosing?
Hoping someone can support my understanding on this topic..
Some papers I read suggest TPH2 expression Increases w/ anxiety/depression, and some suggest expression Decreases. However, from my understanding, a lower serum tryptophan level is associated with these neurological issues, so wouldn't decreased expression make more sense? Unless the increased expression somehow blunts serotonin synthesis?
Journal of the American Chemical SocietyDOI: 10.1021/jacs.0c09576
Qi Ding, Ying Tian, Xin Wang, Ping Li, Di Su, Chuanchen Wu, Wen Zhang, and Bo Tang
https://ift.tt/3l6tI41
Wikipedia states, "The activity of tryptophan hydroxylase (i.e. the rate at which it converts L-tryptophan into the serotonin precursor L-5-hydroxytryptophan) can be increased when it undergoes phosphorylation." I'm wondering if it's possible to promote this phosphorylation.
Im on an SSRI and amphetamines and I want to make sure my brain doesn't deplete too much of serotonin and other neurotransmitters and melatonin. I've read that 5htp is a risk to take for the chance of serotonin syndrome, but since tryptophan hydroxylase is the rate limiting factor for 5 htp production, couldnt I theoretically take all the tryptophan I wanted and my body would only make as much 5htp as there was tryptophan hydroxylase available? Also, where does down regulation play into all this? Thanks
I learned that GHB stimulates tryptophan hydroxylase which is why it is a fine drug to use after MDMA, turning the crash into a soft landing and also boosting the production of serotonin after MDMA inhibited it. Now I am wondering if there is an opiate or opioid which has the same effect.
[Updated version of this post]
https://preview.redd.it/710nj580req71.jpg?width=2262&format=pjpg&auto=webp&s=5f24839f9622c3acb7ac3c832650919f54b3d715
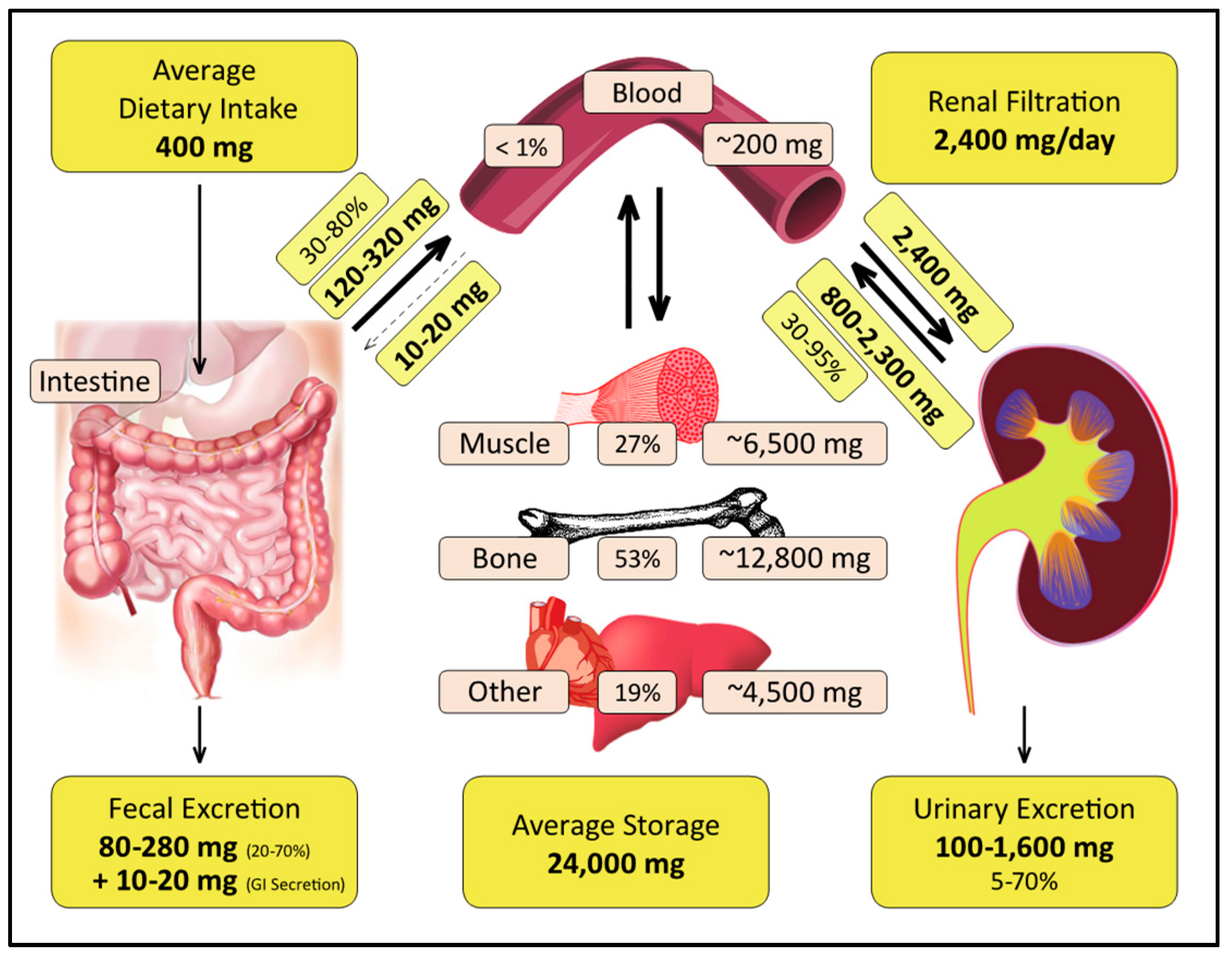
>In humans, red blood cell (RBC) magnesium levels often provide a better reflection of body magnesium status than blood magnesium levels. When the magnesium concentration in the blood is low, magnesium is pulled out from the cells to maintain blood magnesium levels within normal range. Therefore, in case of magnesium deficiency, a blood test of magnesium might show normal levels, while an RBC magnesium test would provide a more accurate reflection of magnesium status of the body. For exact estimation of RBC magnesium level, individuals are advised not to consume vitamins, or mineral supplements for at least one week before collection of RBC samples. A normal RBC magnesium level ranges between 4.2 and 6.8 mg/dL. However, some experts recommend aiming for a minimum level of 6.0 mg/dL on the RBC test.
Hello all, This will be my first post on this subreddit, so here's hoping it's cleared and that i haven't overlooked any rules in posting this and reaching out to the community.
So, where to start... Well I've been taking bromantane for a little while now. Mostly throughout this last year, with a few break between for when I'd run out. I Initially began taking it at around 25-50 mg but have plateaued at around 100. I feel confident that tolerance has indeed set in and that with the doses described many here would agree. Moreso, the effect i felt taking it before is night and day to the effect felt now, which frankly at this point can be difficult to discern. Undeterred, i do still place stock in the underlying pharmacological actions taking place when consumed and thus continue to incorporate it into my semi-daily stack.
On to the topic at hand; on the basis of how it works, I've made it habit to follow it with a protein source of some sort, the best of which imo has been a quick milk & brotein mix made in the morning or otherwise some meat(fish soup, carne asada taco, etc)
Unfortunately however, getting what I feel to be the necessary protein required to make the best use of the drug is not always something i can manage and thus, i come to you Reddit to weigh in on the alternative. Since I haven't spelled it out yet, the idea has been that an upregulation of tyrosine hydroxylase and aromatic amino acid decarboxylase provided through supplementation of bromantane would, in theory and in my mind, be the most beneficial when combined with the amino acids those enzymes act to metabolize.
My question is, would it be better for me to supplement directly with Tyrosine, Tryptophan, etc? Would it provide a stronger effect perhaps? Would, for example, there be any benefit to taking tyrosine and phenylalanine such as improved catecholamine release or some such effect i haven't considered, or result even in an increase in an undesirable metabolite I'm not aware of? I ask these things because supplementing directly could provide more control over the rough approximation of precursors I'd get from protein powder or meat, and an increase in phenethylamine might even contribute to some mild aspect of euphoria which i may not be entirely opposed to. Let me hear your thoughts on this conundrum I've presented myself with.
Has anyone used or uses the Tryptophan supplement while using GHB ?? Do you notice any interactions or side effects such as nausea or increased sleepiness ??? I know that GHB increases the production of Dopamine by stimulating the enzyme tyrosine hydroxylase which accelerates the conversion of L-tyrosine to L-dopa and after Dopamine, but also GHB induces an accumulation of Tryptophan or 5-HTP in the body increasing its bioavailability for the brain .... thanks
Do your worst!
I have made a list of drugs that I have seen in qbanks (UW, Amboss) or just FA that are not mentioned in sketchy pharm. Some of them imo are really LY. So here it is:
Cardiovascular
Levosimendan Ivabradine Regadenoson Sacubitril (entresto) Ranolazine Tafamidis (stabilizes TTR tetramer, reduces formation of TTR amyloid)
Immunology
Ixekizumab/secukinumab Vedolizumab (α4-β7 integrin)
Dupilumab (IL4Rα) Canakinumab (IL1B) Belimumab (anti-BAFF) Bezlotoxumab (anti- toxin B C.diff, decreases relapses) Pegademase (ADA analog for SCID) Muromonab (T-cell) Abatacept Guselkumab Imiquimod Ustekinumab Cyclosporine, tacrolimus, sirolimus Daclizumab, basiliximab
Antimicrobials
Carbenicillin Cefaclor(2nd) Cefpodoxime(3rd) Doripenem, ertapenem Mupirocin (isoleucine t-RNA synthetase) Fosfomycin Iodoquinol Nitazoxanide Spiramycin Suramin Melarsoprol Tolnaftate Permethrin Lindane Fumagillin (microsporidium keratoconjuctivitis) Baloxavir
Antimuscarinics
Glycopyrrolate Hyoscyamine, dicyclomine Solifenacine (oxybutynin) Propantheline
Sympathomimetics
Midodrine Mirabegron Phentermine, diethylpropion, benzphetamine (weight loss) Methoxamine = selective α1 agonist
Sympatholytics Guanfacine (clonidine)
Neurology, Ophthalmology
Ranibizumab (VEGF) Apraclonidine, brimonidine (α2) Bimatoprost, latanoprost (PGF2α) Echothiophate Sodium oxybate GHB (for cataplexy in narcolepsy) Glatiramer (MBP analog MS) Nusinersen (SMA) Acamprosate Felbamate (NMDA receptor antagonist, anticonvulsant) Erenumab (anti-CGRP) Baclofen Buspirone
Endocrine
Thiocyanate Perchlorate anions Metyrapone Tesamorelin (GHRH analog)
Burosumab (anti-FGF23 Hypophosphatemic rickets) Telotristat (tryptophan hydroxylase inhibitor, carcinoid syndrome symptoms management) Cosyntropin (ACTH analog) Mitotane
Oncology
Panitumumab (cetuximab) Trametinib (MEK inhibitor) Aldesleukin (IL-2) L-asparaginase Alectinib, crizotinib Abiraterone Olaparib
Hematology
Andexanet alfa (inactivated recombinant factor Xa) Idarucizumab Senicapoc (Gardos channel blocker, sickle cell disease) Bortezomib (proteasome inhibitor) Panobinostat, Vorinostat (HDAC inhibitors) Dasatinib (imatinib) Ruxolitinib (JAK1/2) Fostamatinib (macrophage inhibitor in ITP) Luspatercept (β thalassemia, MDS) Oprelvekin (IL-11) Eltromobag, romiplostim Venetoclax Emicizumab Voxelotor Lenalidomide Azacitidine Eculizumab
Respiratory
Mepolizumab, Reslizumab (IL-5, asthma) Benralizumab (IL-5R) Pirfenidone Nintentani
... keep reading on reddit ➡For context I'm a Refuse Driver (Garbage man) & today I was on food waste. After I'd tipped I was checking the wagon for any defects when I spotted a lone pea balanced on the lifts.
I said "hey look, an escaPEA"
No one near me but it didn't half make me laugh for a good hour or so!
Edit: I can't believe how much this has blown up. Thank you everyone I've had a blast reading through the replies 😂
I've been on SSRI's for many years and ended up at a low dose. However, in the past 6 months I felt depressed, tired, angry, irritable etc. all the time. I also started looking much more tired and my sleep was bad. My doctor and I tried to increase SSRI dose, to no effect. Then I ended up deciding to quit it since I suspected it wasn't doing much. It gave a bit more energy but 1-2 weeks in my anger/depression issues became really bad. Working from home all the time due to covid, but I could get so angry over various things co-workers did I would be so tense in my neck, head, brain etc. I actually became sore from it after. I felt I was going crazy and should maybe call in sick for a month and move to a hotel. Anyway, as a last ditch thing I decided to quit coffee since I believe I read it lowered serotonin (by inhibiting tryptophan hydroxylase) which was probably not good given the low-serotonin after quitting the SSRI. It was tough for two days but now just a week after than I feel better than I have in over a year. I sleep longer and I have much more neergy. All the anger and neck/head tension issues are completely gone. It even seems I've lost a bit of wait (not that I was fat but I have some corona padding). I somehow feel the caffeine has been completely fucking with everything. Feels good to be off everything, caffeine and SSRI, now!
They’re on standbi
Pilot on me!!
Dad jokes are supposed to be jokes you can tell a kid and they will understand it and find it funny.
This sub is mostly just NSFW puns now.
If it needs a NSFW tag it's not a dad joke. There should just be a NSFW puns subreddit for that.
Edit* I'm not replying any longer and turning off notifications but to all those that say "no one cares", there sure are a lot of you arguing about it. Maybe I'm wrong but you people don't need to be rude about it. If you really don't care, don't comment.
What did 0 say to 8 ?
" Nice Belt "
So What did 3 say to 8 ?
" Hey, you two stop making out "
I won't be doing that today!
You take away their little brooms
This morning, my 4 year old daughter.
Daughter: I'm hungry
Me: nerves building, smile widening
Me: Hi hungry, I'm dad.
She had no idea what was going on but I finally did it.
Thank you all for listening.
There hasn't been a post all year!
It’s pronounced “Noel.”
After all his first name is No-vac
What, then, is Chinese rap?
Edit:
Notable mentions from the comments:
Spanish/Swedish/Swiss/Serbian hits
French/Finnish art
Country/Canadian rap
Chinese/Country/Canadian rock
Turkish/Tunisian/Taiwanese rap
There hasn't been a single post this year!
(Happy 2022 from New Zealand)
I learned that GHB stimulates tryptophan hydroxylase which is why it is a fine drug to use after MDMA, turning the crash into a soft landing and also boosting the production of serotonin after MDMA inhibited it.
Now I am wondering if there is an opiate or opioid which has the same effect.
[Updated: Sep 23, 2021: Added charts and new Video Links]
\"50% of the population does not get adequate magnesium\"
Original Source: How Vitamin D And Magnesium Work Together | Mark Hyman, MD [Mar 2020]
>In humans, red blood cell (RBC) magnesium levels often provide a better reflection of body magnesium status than blood magnesium levels. When the magnesium concentration in the blood is low, magnesium is pulled out from the cells to maintain blood magnesium levels within normal range. Therefore, in case of magnesium deficiency, a blood test of magnesium might show normal levels, while an RBC magnesium test would provide a more accurate reflection of magnesium status of the body. For exact estimation of RBC magnesium level, individuals are advised not to consume vitamins, or mineral supplements for at least one week before collection of RBC samples. A normal RBC magnesium level ranges between 4.2 and 6.8 mg/dL. However, some experts recommend aiming for a minimum level of 6.0 mg/dL on the RBC test.
Please note that this site uses cookies to personalise content and adverts, to provide social media features, and to analyse web traffic. Click here for more information.










{kind=link}